Shoulder conditions -Private treatment in London
The shoulder is the most mobile joint in the body, which makes it one of the most vulnerable to injury, degeneration, and pain.
Mr Toby Baring is a consultant orthopaedic surgeon specialising exclusively in shoulder and elbow conditions, seeing patients at One Welbeck, King Edward VII's Hospital, and the Hospital of St John and Elizabeth in London.


Is this right for you?
Persistent shoulder pain that hasn't improved with rest or physiotherapy
Pain at night that disrupts your sleep, particularly lying on the affected side
A grinding, clicking, or catching sensation when you move your arm
Weakness in the shoulder following an injury or that has developed gradually over time
A previous shoulder operation that hasn't delivered the expected result
Conditions treated
Mr Baring diagnoses and treats the full range of shoulder conditions, including:
Rotator cuff tears — partial and full thickness tears, managed with keyhole surgery or structured rehabilitation
Frozen shoulder (adhesive capsulitis) — hydrodilatation injections and keyhole capsular release
Shoulder arthritis — from steroid injections through to anatomic and reverse shoulder replacement
Shoulder instability — dislocation, subluxation, and ligament reconstruction
Shoulder impingement — subacromial decompression and bursitis treatment
AC joint problems — acromioclavicular joint injuries and arthritis
Fractures and trauma — proximal humerus fractures and clavicle injuries

Approach
Mr Baring takes a conservative-first approach wherever appropriate, not every shoulder condition requires surgery.
A thorough assessment, including clinical examination and imaging where needed, will identify exactly what is causing your symptoms and what is most likely to resolve them. Where surgery is recommended, Mr Baring uses minimally invasive keyhole techniques wherever possible to reduce recovery time and post-operative discomfort.

View all conditions we treat
Recovery Timeline
Highly variable by case, recovery depends entirely on the complexity of the revision. Mr Baring will give you a realistic timeline at your consultation.
Non-surgical treatment - Physiotherapy and injections: improvement typically within 6–12 weeks
Keyhole surgery - Return to light activities in 2–4 weeks; full recovery 3–6 months depending on procedure
Shoulder replacement - Hospital 1–2 nights; sling for 6 weeks; most patients reach full recovery by 6 months
We work with the following insurers
If you don't see your insurer listed please reach out and we will chat through the options with you.









Featured services
View all services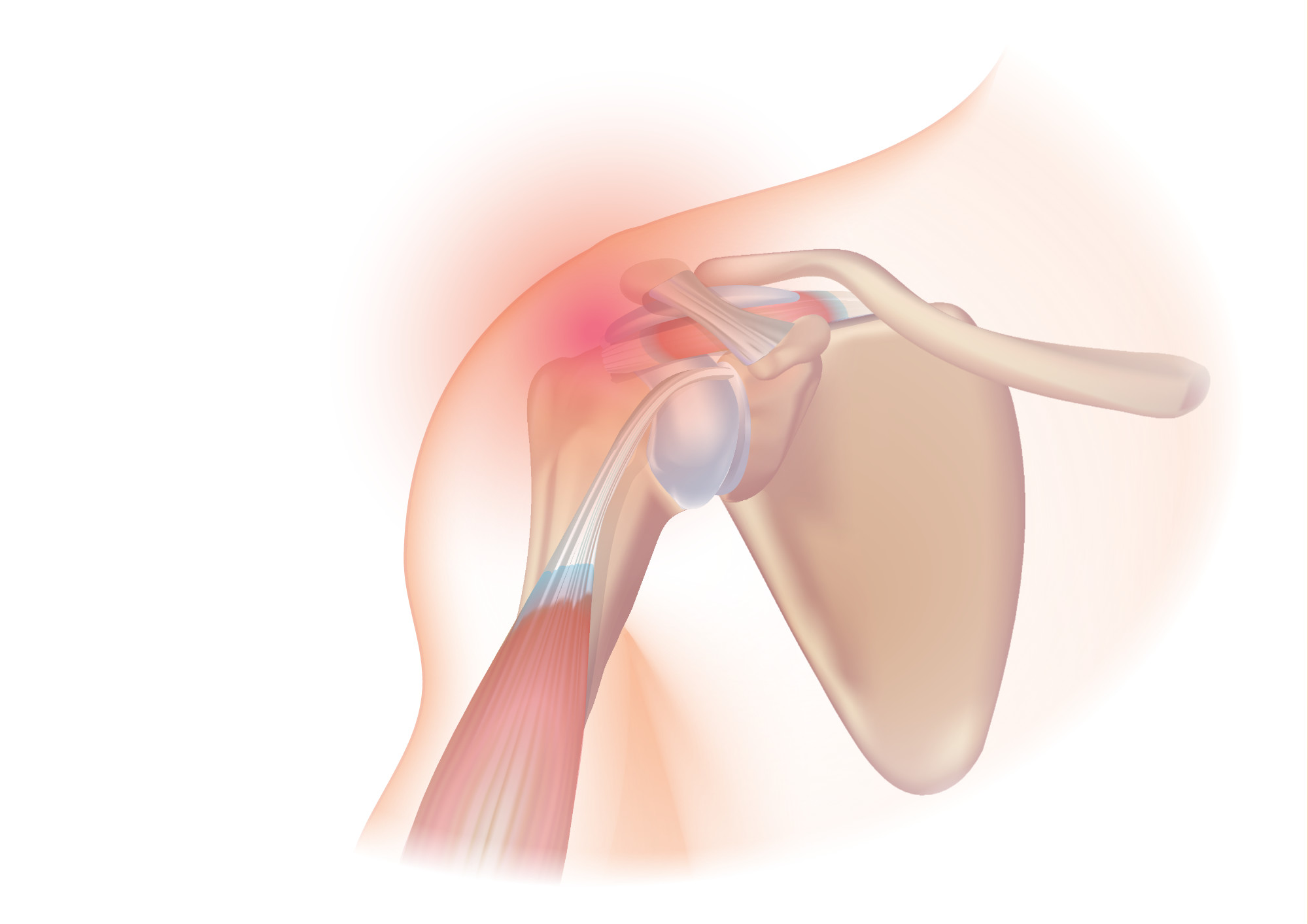
Shoulder replacement
Restore your movement and eliminate arthritic pain. Specialist anatomic and reverse shoulder replacement with Mr Toby Baring. Seeing patients at King Edward VII and OneWelbeck.
Rotator Cuff Repair
Stop living with shoulder pain. Expert minimally invasive (keyhole) surgery and rapid recovery with
Mr Toby Baring in central London.

Frozen shoulder treatment
Stop the stiffness and regain your sleep. Rapid assessment, hydrodilatation injections, and keyhole release surgery with Mr Toby Baring in central London.
Customer testimonials
Some of the nice things people have said about us.
My recovery was fast, which attests to Dr Baring's expertise in shoulder surgery.
Highly recommendable specialist with a great support team.
He has also taken an interest in my health generally; he has gone to the trouble of finding for me a specialist for another problem. I cannot speak more highly of his care.
Locations
The locations you can meet Mr Toby Baring for Consultation or Surgery.



FAQs
Commonly asked questions about Frozen Shoulder in London
The most common cause in adults over 40 is rotator cuff degeneration, the gradual wearing of the tendons that power and stabilise the shoulder joint. This can range from tendon inflammation (tendinopathy) to partial or full thickness tears. Other common causes include frozen shoulder, shoulder impingement, and acromioclavicular joint arthritis. In younger, more active patients, instability from previous dislocation is a frequent presentation. An accurate diagnosis is essential before treatment, the right approach for a rotator cuff tear is very different from the right approach for frozen shoulder.
Not necessarily. In many cases Mr Baring can make an accurate clinical assessment at your first appointment without prior imaging. If a scan is needed, he will arrange an MRI or X-ray — usually at the same hospital where you are being seen, on the same day or shortly after. If you already have recent imaging from a GP or another specialist, bring it with you — it will help inform the consultation and may avoid the need for repeat scans.
Surgery is generally considered when non-surgical treatment, physiotherapy, injections, activity modification, has been tried for an appropriate period and has not produced sufficient improvement, or when the nature of the injury makes conservative management unlikely to succeed. Some conditions, such as significant rotator cuff tears in active patients or advanced arthritis, are more likely to benefit from surgical intervention. Mr Baring will give you an honest assessment of the evidence for your specific condition, including what surgery is likely to achieve and what the alternatives are.
Yes. Pain that appears to originate in the shoulder can sometimes be referred from the neck (cervical spine), particularly if you also have symptoms such as pain or tingling that travels down the arm. Occasionally, conditions such as heart disease or gallbladder problems can refer pain to the shoulder region. Mr Baring will assess your symptoms carefully to determine whether your pain is intrinsic to the shoulder joint or has another source , this is an important step that is sometimes missed in a rushed assessment.
Still have questions?
Get in touch below and we'll be able to help you.
Start your recovery today.
Book a consultation today. Appointments available this week.
