If your shoulder keeps giving way, or you've had a dislocation and are wondering what comes next, here's an honest look at instability, when physiotherapy is enough, and when it isn't.


There's a particular kind of anxiety that comes with shoulder instability. It's not always constant pain, it's the moment of hesitation before you reach for something on a high shelf, or the split second during a rugby tackle or a swim stroke when you feel the shoulder shift and wonder if this is the time it goes again.
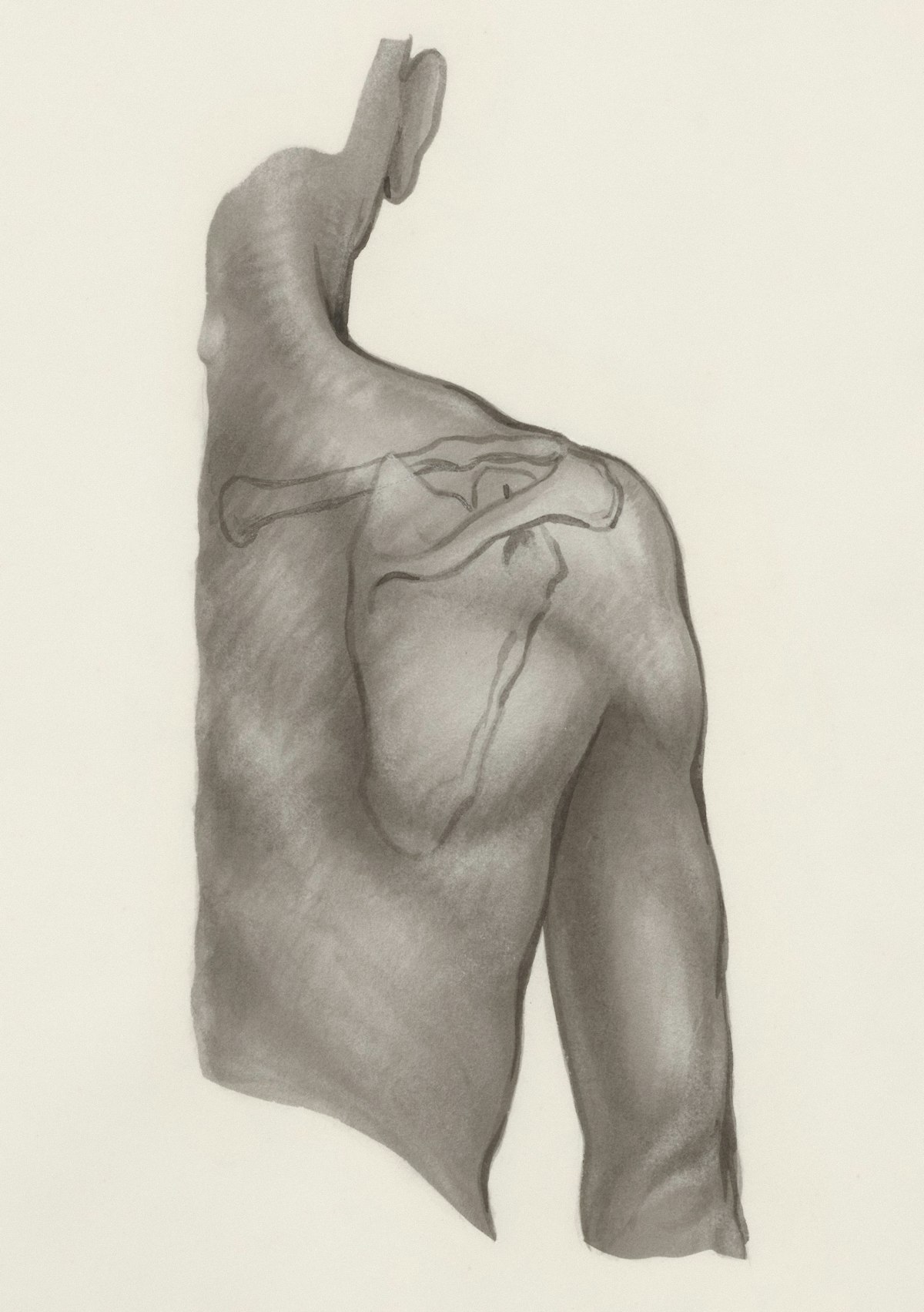
The shoulder is a ball-and-socket joint with an enormous range of motion, which makes it useful but also inherently vulnerable. Stability comes from a combination of the labrum (a ring of cartilage that deepens the socket), the joint capsule, and the surrounding muscles. When any of those structures are damaged or insufficient, the ball can slip partially out of the socket (a subluxation) or fully out (a dislocation).
Shoulder instability isn't one condition, it's a spectrum. Some patients come in after a single traumatic dislocation wanting to understand their options. Others have had the shoulder "go" dozens of times and are at the point where it happens during everyday activity or even in bed. Others have never had a frank dislocation but live with a constant sense that the shoulder isn't right.
This distinction matters because it changes the treatment pathway considerably.
Traumatic instability follows a specific event: a fall, a collision in sport, an awkward movement that forces the shoulder beyond its limits. The most common result is a Bankart lesion, where the labrum peels off the front of the socket. The joint capsule is usually stretched or torn at the same time. Once that structural damage has occurred, the shoulder is vulnerable to going again.
Atraumatic instability develops without a single precipitating injury. It's more common in people with generalised joint hypermobility, and it tends to affect the shoulder in multiple directions rather than just one. The treatment approach here is quite different, physiotherapy and muscle strengthening are the starting point, and surgery is less often the right answer.
Understanding which category applies to you is one of the first things I work through at a consultation.
Learn more about other shoulder conditions here.
For traumatic anterior instability, the honest answer is: quite likely, particularly if you're young and active.
In patients under 25 who return to sport after a first dislocation without surgery, recurrence rates are high. A landmark 25-year prospective study by Hovelius et al. found a 72% recurrence rate in patients aged 12 to 22 managed non-operatively. In contact athletes and military populations, rates in some series exceed 90%. The risk drops with age but remains significant throughout the third decade.
Citation: Hovelius L, et al. J Bone Joint Surg Am. 2008;90(5):945–952. PMID: 18451384
The other thing worth knowing is that each subsequent dislocation typically causes a little more damage. The labrum tears further. Bone is lost from the front of the socket (a bony Bankart) or from the back of the ball (a Hill-Sachs lesion). Once bone loss becomes significant, the surgical options become more complex. This is why many surgeons, myself included, advocate for earlier assessment in young active patients rather than waiting to see how many times it happens.
Physiotherapy has a genuine role in shoulder instability management, but its effectiveness depends entirely on the type of instability.
For atraumatic and multidirectional instability, a structured programme focusing on rotator cuff strengthening and scapular control can make a substantial difference. These patients often do well without surgery and should try physiotherapy first.
For traumatic instability with a structural Bankart lesion, physiotherapy can improve muscle support around a damaged joint, but it cannot reattach a torn labrum. The cartilage will not heal back to the bone on its own. Physio can reduce symptoms and delay further episodes, but it doesn't change the underlying structural problem.
If you've done a thorough course of physiotherapy and your shoulder is still giving way, that's important information, not a reason to try more of the same.
These situations suggest a specialist review makes sense rather than continuing to manage:
This is the standard surgical treatment for traumatic anterior instability where the labrum is torn and there is no significant bone loss. Using keyhole incisions and a camera, the labrum is reattached to the front rim of the socket using small anchors. The capsule is tightened at the same time.
In low demand patients who do not play contact or overhead sports, over the age of 30, this procedure maintains stability of the shoulder long term in about 85% of patients. It's done under general anaesthetic as a day case, and most patients go home the same day.
Historically these were procedures reserved for revision surgery when a Bankart had failed or when there was severe bone loss from the front of the socket. Improved understanding of instability and appreciation that Bankart repairs have a high failure rate in younger more active patients has led to a move to bone block procedures. These involve attaching a block of bone graft to the front of the socket to physically block the ball from dislocation. The block of bone is held in place with screws or, more recently, metal buttons while it heals into place. Due to the rapid healing of bone, recovery is accelerated compared to soft tissue procedures.
Posterior instability is less common but does occur, usually in overhead athletes or following specific trauma. The principles are similar to anterior stabilisation — repair of the posterior labrum and capsule. The approach and recovery are comparable to a Bankart repair.
After a Bankart repair, you'll be in a sling for four to six weeks. Physiotherapy begins early with gentle range of motion, progressing to strengthening from around six weeks. Most patients are back to non-contact sport by four to six months, and contact sport at six to nine months.
Bone block procedures have a quicker recovery and return-to-sport timeline is similar. Imaging (CT scan) is often performed to assess bone healing around six weeks, and if this is progressing, which it is in 90% of cases, patients move onto a graduated return to all activities over the next two to three months. Full recovery takes between three to four months, including return to contact sports.
I'll take a full history of how the instability started, how many episodes you've had, which direction the shoulder goes, and how it's affecting your life. I'll examine the shoulder with specific stability tests and review any existing imaging.
If you haven't had an MRI, I'll usually arrange one. For patients where bone loss is a possibility, a CT scan gives more reliable information than MRI alone. By the end of the appointment you'll have a clear picture of what's going on and a treatment recommendation that's specific to your situation.

For atraumatic and multidirectional instability, yes — physiotherapy resolves the problem for many patients. For traumatic instability with a structural Bankart lesion, the labrum will not reattach on its own, so while symptoms can be managed, the underlying vulnerability remains without surgical repair. However, a proportion of people who dislocate once do not have a further episode, even without surgery, and this increases with age.
No. Subluxations (partial shifts where the shoulder doesn't fully come out) are still significant events and can cause the same structural damage over time. Apprehension — the feeling that the shoulder might go, even if it hasn't, is also a recognised symptom worth investigating.
Bone loss isn't always visible on a standard MRI. If there's any suspicion based on the number of previous dislocations or the clinical picture, a CT scan is the more reliable investigation. This is something I assess at the first consultation and arrange if needed before making a surgical recommendation.
Age is rarely a reason not to operate. The decision is based on the number of episodes, your activity level, and what you want to be able to do. Younger active patients are often the clearest candidates for early surgery given the high recurrence rates without it. Older patients are assessed individually, a first dislocation over 40 would typically prompt an MRI to check the rotator cuff has not been damaged alongside the labrum before deciding on the approach.
If your shoulder has been giving way, or you've had more than one dislocation, a single consultation is usually enough to understand what's happening and what to do about it.